

{kind=link}
{kind=link}
{kind=link}
{kind=link}
-

Incidence of Symptomatic Upper Extremity Deep Vein Thrombosis in Respect to Subcutaneous Port Venous Access Site in Adults: A Retrospective Review
Catherine Bark, Alexsandra Biel, Corinne G. Bowditch, Paul Bove, and Jimmi Mangla
Publication Date: 5-2024
Subcutaneous ports are an essential component of care in patients who require long-term central venous access and are commonly indicated for patients that require chemotherapy, infusions, intravenous (IV) antibiotics or frequent blood draws.1,2 The catheter of the subcutaneous port is commonly inserted through the subclavian vein and internal jugular vein via percutaneous insertion, or the external jugular vein and cephalic vein via surgical cutdown of the vein.
One of the most common port-related complications is venous thromboembolic (VTE) events with rates of symptomatic VTE as high as 13.6%.4,6–11 Patients with symptomatic upper extremity deep vein thrombosis (DVT) can present with symptoms of ipsilateral arm or neck swelling, pain, and erythema.
The purpose of this study is to evaluate the rate of symptomatic upper extremity deep vein thrombosis based on the subcutaneous port venous access site.
-

Trends in Thoracic Endovascular Aortic Repair in Patients 45 Years Old and Younger
Brandon Diaz, Alexander Chen, Graham W. Long, Rose Callahan, Diane Studzinski, and Otto W. Brown
Publication Date: 3-2024
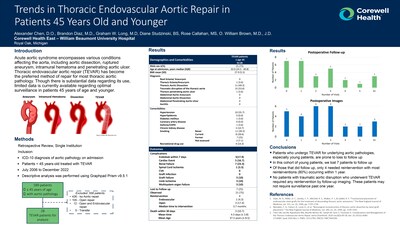
Objective:Thoracic endovascular aortic repair (TEVAR) is now the preferred method of repair for most aortic pathology. This report explores the indications, morbidity, and long-term implications of TEVAR in patients under 45 years old.
/="/">Methods:This is a retrospective, single-institution study of electronic medical records for all patients under age 45 years treated with TEVAR from July 2006 to December 2022. Data collected included demographics, comorbidities, and 30-day and long term outcomes, including medical and aortic-related complications.
/="/">Results:The study cohort consisted of 30 patients, mean age 32 years, 22 males (73.3%), 10 (33.3%) with hypertension, and 15 (50%) were smokers. There were 16 (53.3%) traumatic disruptions, 1 (3.3%) aneurysm, 1 (3.3%) penetrating atherosclerotic ulcer, and 12 (40%) dissections (7 Type A and 5 Type B). Three patients died within 30 days of their procedure for a perioperative mortality rate of 10%; the interval from procedure to death was a mean 4.3 days (SD ± 3.8). Twenty-one had at least 1 follow-up visit post-TEVAR and 22 underwent at least one follow-up imaging study. Thirty-day morbidity overall was 50% and included endoleak in 6 (20%), cardiac complications in 5 (16.7%), renal failure in 7 (23.3%), spinal cord ischemia in 1 (3.3%), graft failure in 1 (3.3%), limb ischemia in 3 (10%), and multi-system organ failure in 3 (10%). Of the 22 patients with follow-up imaging, endovascular reinterventions were required in 4 (18.2%), while open surgical reintervention was necessary in 1 (4.5%). Reinterventions occurred at a median of 3.7 months postoperatively (0.7-60.8) and were indicated for 1 expanding aneurysm, 3 endoleaks, and 1 for combined endoleak and expanding aneurysm. There was one late death at 1.1 months (aortic-related) and another deceased patient whose cause and date of death are unknown.
/="/">Conclusion: Historically, patients that undergo TEVAR for underlying aortic pathologies, especially young patients, are followed long-term to monitor for further aortic degeneration and possible reintervention. In our study, majority of all reinterventions (80%) occurred within 1 year. However, all patients with traumatic aortic disruption who underwent TEVAR did not require any reintervention upon follow-up imaging. These patients may not require surveillance past one year -

Utility of Great Saphenous Vein Mapping in the Detection of Superficial Vein Thrombosis Prior to Infrainguinal Arterial Bypass
Melissa C. Hetrick, Ashley E. Beale, Graham W. Long, Sarvar Oreizi-Esfahani, Rose E. Callahan, Diane M. Studzinski, and Otto W. Brown
Publication Date: 3-2024
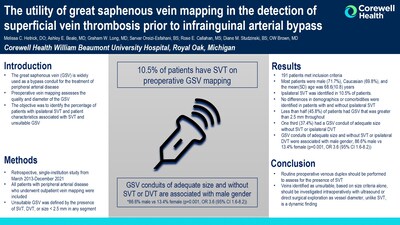
OBJECTIVE: The great saphenous vein (GSV) is widely used as a bypass conduit for the treatment of infrainguinal peripheral arterial disease. Preoperative vein mapping assesses both the quality and diameter of the GSV. Ultrasound findings regarded as unfavorable are the presence of superficial vein thrombosis (SVT), ipsilateral deep vein thrombosis (DVT), and small vessel diameter. Identifying a suitable conduit is of utmost importance as GSV bypasses have improved patency compared to alternative conduits. The primary objective of this study was to identify the percentage of patients with ipsilateral SVT as well as patient characteristics associated with SVT and unsuitable GSV.
/="/">METHODS: Retrospective, single-institution study from March 2013-December 2021. All patients with peripheral arterial disease who underwent outpatient vein mapping were included. Unsuitable GSV was defined by the presence of SVT, DVT, or size < 2.5 mm in any segment (from proximal thigh to distal calf).
RESULTS: A total of 191 patients met inclusion criteria. Most patients were male (71.7%), Caucasian (69.8%), and the mean(SD) age was 68.6(10.8) years. Ipsilateral SVT was identified in 10.5% of patients. No significant differences in demographics or comorbidities were identified in patients with and without ipsilateral SVT. Less than half (45.8%) of patients had GSV that was greater than 2.5 mm throughout, and only one third (37.4%) had a GSV conduit of adequate size without SVT or ipsilateral DVT. GSV conduits of adequate size and without SVT or ipsilateral DVT were associated with male gender, 86.6% male vs 13.4% female (p=0.001, OR 3.6 (95% CI 1.6-8.2)). After completion of vein mapping, 90 (62.1%) patients underwent infrainguinal bypass and the ipsilateral GSV was used as a conduit in 58.9% of cases.
/="/">CONCLUSIONS: Our study revealed that 10.5% of patients have SVT identified on preoperative vein mapping. Given these findings, routine preoperative venous duplex should be performed to assess for the presence of SVT, as this finding is difficult to identify intraoperatively and may predict lower patency rates. Veins identified as unsuitable, based on size criteria alone, should still be investigated intraoperatively with ultrasound or direct surgical exploration as vessel diameter, unlike SVT, is a dynamic finding. -

A Penetrating Neck Injury Resulting in Complete Transection of the Ipsilateral Common Carotid Artery, Delayed Contralateral Pneumothorax and Occult Esophageal Injury: A Case Report with a Multidisciplinary Approach to Management
Michaela Knaggs, Christian Przeslawski, Peter Habib, Ahmed Ghamraoui, Caitlin Wahl, and Jeffrey Gerken
Publication Date: 5-4-2023
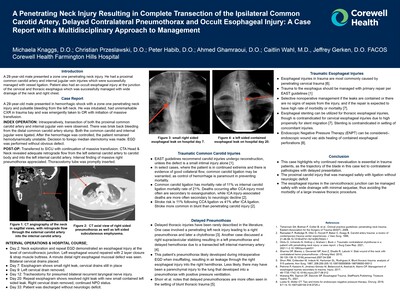
A 29-year-old male presented a zone one penetrating neck injury. He had a proximal common carotid artery and internal jugular vein injuries which were successfully managed with vessel ligation. Patient also had an occult esophageal injury at the junction of the cervical and thoracic esophagus which was successfully managed with wide drainage of the neck and right chest.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.