

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
-

Diagnosis and Management of Acute Chest Syndrome
Zachary Awad, Hashem Mohilldean, Nataly Salman, and Roy Soto
Publication Date: 10-20-2024
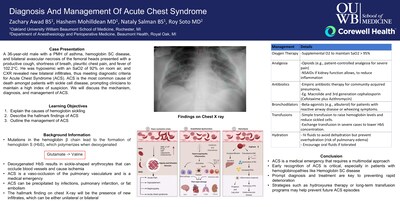
A 36-year-old male with a PMH of asthma, hemoglobin SC disease, and bilateral avascular necrosis of the femoral heads presented with a productive cough, shortness of breath, pleuritic chest pain, and fever of 102.2°C. He was hypoxemic with an SaO2 of 92% on room air, and CXR revealed new bilateral infiltrates, thus meeting diagnostic criteria for Acute Chest Syndrome (ACS). ACS is the most common cause of death amongst patients with sickle cell disease, prompting clinicians to maintain a high index of suspicion. We will discuss the mechanism, diagnosis, and management of ACS.
-

Elimination Of Postoperative Narcotics In Infant Robotic Pyeloplasty Using Caudal Anesthesia And A Non-Narcotic Pain Pathway
Kwesi Asantey, Kristen Meier, Zachary Rollins, Andrew B. Banooni, and Zachary J. Liss
Publication Date: 5-2-2022
INTRODUCTION
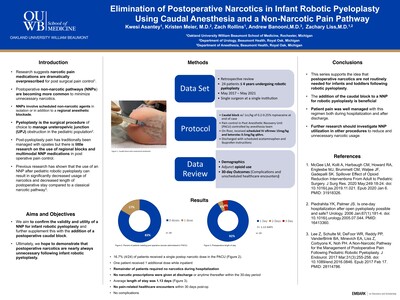
Research suggests that narcotic pain medications are dramatically overprescribed. We hypothesize that narcotics are unnecessary in the majority of infants for postoperative pain control. In this series, we report our experience combining caudal blocks with a non-narcotic postoperative pathway as a means of completely eliminating postoperative narcotics following infant robotic pyeloplasty. -

ERAS vs Non-ERAS: A Hospital Performance Metrics Comparsion in Patients Undergoing Spinal Fusion
Richard W. Easton, Gregory Smith, Matthew Lipphardt, Nai-Wei Chen, Pestano Cecile, Hermeli Mateo, Austin Ahlgren, Brady Vibert, Andrew Sagante, and Susan Vander Beek
Publication Date: 5-2022
Hospital metrics are measures used to evaluate surgical quality. The goal is to improve standards of care (SOC). Hospital performance is made publicly available and has reimbursement ramifications.
-

Intraoperative MAP, Vasopressors, and Opioids in TF-TAVR patients undergoing Conscious Sedation vs General Anesthesia
Brett J Friedman, Patrick Karabon, and Wei C Lau
Publication Date: 5-2-2022
INTRODUCTION
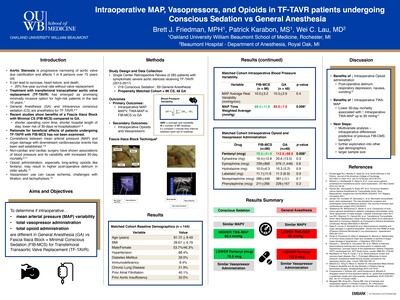
Aortic stenosis is a progressive narrowing of the aortic valve that can cause serious cardiovascular harm such as syncope, heart failure, and death if left untreated. Transfemoral-transcatheter aortic valve replacement (TF-TAVR) emerged in the last 10 years as an alternative for previously inoperable, high-risk patients. Studies suggest that monitored anesthesia for TF-TAVR using minimalist conscious sedation results in better outcomes (e.g., shorter length of stay, lower 30-day mortality) when compared to general anesthesia. However, there is a gap in knowledge of why conscious sedation is more successful. Recent studies have demonstrated the association of intraoperative mean arterial pressure (MAP) variables including MAP variability (MAPV) and time-weighted average MAP (TWA-MAP) with 30-day mortality in non-cardiac surgery. We compared intraoperative variables for TF-TAVR patients that underwent conscious sedation versus general anesthesia. -

Intussusception- a rare cause of non-specific chronic pain: a case report
Nasim Shakibai and Rebecca Clemans
Publication Date: 11-19-2022
Introduction:
Non-specific chronic pain is difficult to treat, especially in a patient with a complex medical history and pain in multiple regions of the body. It is important to use a multidisciplinary approach in treating such patients. In addition, it is necessary to be aware of conditions that are often non-specific in presentation such as intussusception. We describe a case report of a patient with non-specific chronic pain that was found to have intussusception.
Case Report:
A 42-year-old female with a past medical history of gastric adenocarcinoma status post gastrectomy with Roux-en-Y, chemotherapy that was completed the year before and left salpingo-oophorectomy for metastatic gastric carcinoma. She initially presented to the chronic pain management clinic with lower back pain for several years after failed conservative treatment. She was diagnosed with sacroiliitis and subsequently underwent bilateral sacroiliac injections of 40mg Kenalog in addition to 3ml of 0.25% Bupivacaine, which did not resolve her pain. Two weeks later, she presented to the emergency department with the chief complaint of worsening upper chest and shoulder pain that radiated to the inferior aspect of her left scapula over the past three days. Chest x-ray, troponins and EKG were all within normal limits. She was then discharged home.
Five days later, she presented with lower abdominal pain that had been persistent for the past year and left flank pain/back pain for the past four months that suddenly became intolerable. She continued to endorse post-prandial nausea, vomiting with chronic constipation. On physical examination, she had tenderness to palpation of the left lower quadrant without rebound, guarding or distention. She also had tenderness to palpation of the left flank.
A whole-body positron emission tomography computed tomography (CT) and an ultrasound of the kidneys and bladder done at this admission were negative. Previous MRI of the lumbar spine, bone scan and small bowel series were negative. Urine analysis and post-void residual were negative. CT of the abdomen with IV contrast, as shown in Figure 1, demonstrated segmented jejunojejunal intussusception with edematous bowel wall. She subsequently underwent an exploratory laparotomy with reduction of a retrograde intussusception wand bilateral transversus abdominis plane blocks. No obvious mass or lead point were identified. In her follow-up appointment, her abdominal, flank and back pain were minimal and she was improving overall.
Discussion:
Intussusception is a common cause of intestinal obstruction in children but is a rare cause in adults. Due to its non-specific presentation, it is difficult to diagnose. Some patients present with chronic or intermittent vague abdominal pain with nausea and vomiting, abdominal distension with partial obstruction, and rarely a palpable mass on physical examination. [1] While it is often idiopathic in children, adults often have a lead point to indicate another condition. Some of the causes include inflammatory bowel disease, previous Roux-en-Y, inflammatory fibroid polyp, postoperative adhesions, Meckel’s diverticulum, benign and malignant lesions and jejunostomy feeding tubes. [1,2,3] With an increase in Roux-en-Y surgeries, there has been an increase in intussusception as a complication. [4]
Ultrasounds are useful in the diagnosis of intussusception but CT with IV contrast is the most useful diagnostic tool for the evaluation of intussusception. Surgery is the definitive treatment for adult intussusception.
As we treat patients with chronic pain that do not have an improvement with conservative treatment in addition to more invasive treatment such as glucocorticoid injections, there needs to be a workup for medical conditions in the rare case that they are the cause.
-

What is the Incidence of QT Prolongation and Life-Threatening Arrhythmia Following IV Methadone Administration in Patients Undergoing Lumbar Fusion?
Gregory Smith, Richard W. Easton, Kuldeep Shah, Daniel Silvasi, Matthew Lipphardt, Julie George, Shengchuan Dai, Brian Williamson, Brady Vibert, Bradley Ahlgren, and Nicholas Papakonstantinou
Publication Date: 5-2022
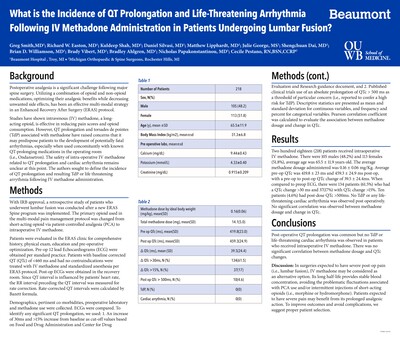
Postoperative analgesia is a significant challenge following major spine surgery. Utilizing a combination of opioid and non-opioid medications, optimizing their analgesic benefits while decreasing unwanted side effects, has been an effective multi-modal strategy in an Enhanced Recovery After Surgery (ERAS) protocol.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.